

Feeding a child with complex allergies? The Recipe Resource is full of recipes and useful tips.
Monday, 24 December 2012
Genius Christmas Heroes!
My twins are Genius Gluten Free's "Christmas Heroes " for Christmas Eve :) and were delighted to receive a box of goodies including the most delicious mince pies which got the thumbs up from us!

Saturday, 17 November 2012
Marmite Pinwheels
A friend asked for this very simple recipe after her son enjoyed them so much at our house recently!
It's so easy (and quick) but they don't keep very well due to the usual problems with "free from" pastry mix.

Method
- Using a pastry mix, (such as Crimble's pastry or mix up the Juvela Harvest White bread mix as per the pastry recipe on the back of the box.) make up a ball of pastry.
- Roll out and spread with Marmite. (Not suitable for coeliacs sadly)
- Cut into strips and roll up, then cut the cylinder into rounds.
- Bake for 7-10 mins until the pastry is cooked.
Tip: Free From pastry can get very dry, warming for a few seconds in the microwave before eating is recommended.
Update on the VEGG
OK, I've (finally) been experimenting. I have finally completed a full range of recipe tests with the VEGG and here are my results:-
As an egg replacer in a cake recipe - makes for a soggier mixture. I mixed up the VEGG mixture and added the equivalent weight to the mixture. A regular sponge cake would expect 4oz of sugar, 4oz of flour and 4oz or 2 whole eggs. (The weight equivalent was something I was rather slow to realise!!)
I think 3oz of VEGG mixture would have done. It rose well, tasted fine but was a little dense and wet.
As a quiche filling - Epic fail. Sorry VEGG makers but it looks awful, didn't set until 24 hrs later in the fridge and even I - who can quite happily try almost anything - struggled to taste it. Not good. Now I suspect if I wasn't making a plain quiche it might be considerably better, but my fussy kids won't entertain anything in the mixture so it probably wasn't an entirely fair test. All went in the bin though...
As "Eggy Bread" - very successful, I do recommend this one. Soak bread in the VEGG mixture and then fry. Worked a treat.
As scrambled egg - Hmmmm not convinced. It goes a little "seaweed like" in texture/appearance. Can't explain it but the appearance put us off. Try it an see!
More info and advice from the VEGG peeps themselves here. I think you might see what I mean about the "seaweed" in the picture on their site!

As an egg replacer in a cake recipe - makes for a soggier mixture. I mixed up the VEGG mixture and added the equivalent weight to the mixture. A regular sponge cake would expect 4oz of sugar, 4oz of flour and 4oz or 2 whole eggs. (The weight equivalent was something I was rather slow to realise!!)
I think 3oz of VEGG mixture would have done. It rose well, tasted fine but was a little dense and wet.
As a quiche filling - Epic fail. Sorry VEGG makers but it looks awful, didn't set until 24 hrs later in the fridge and even I - who can quite happily try almost anything - struggled to taste it. Not good. Now I suspect if I wasn't making a plain quiche it might be considerably better, but my fussy kids won't entertain anything in the mixture so it probably wasn't an entirely fair test. All went in the bin though...
As "Eggy Bread" - very successful, I do recommend this one. Soak bread in the VEGG mixture and then fry. Worked a treat.
As scrambled egg - Hmmmm not convinced. It goes a little "seaweed like" in texture/appearance. Can't explain it but the appearance put us off. Try it an see!
More info and advice from the VEGG peeps themselves here. I think you might see what I mean about the "seaweed" in the picture on their site!

Thursday, 8 November 2012
47 Sleeps until Christmas!
With Christmas only 7 weeks away I thought I would post about some free from Christmas treats for children. If you are looking for something a little more special at Christmas, Hotel Chocolat are to be highly recommended. They carefully label their products and cater for dietary needs. Their vegan range is particularly good, my favourite this year is the "Tiddly" range - especially the penguins!



Not necessarily the cheapest free from chocolate, but SO tasty. They also stock an Advent Calendar this year. Don't be put off by their lack of "Free From" labels, they have excellent customer service and speedy delivery. Full marks in our house!

Sunday, 28 October 2012
Fabulous Flapjack update!!!!
Since my daughter was required to be gluten free, on top of the dairy, soya and wheat restriction, we have struggled to find a way of making flapjacks which look "right" and hold together. After months of trials (with very willing taste testers!!) my wonderful mother (who used to teach Domestic Science and is a wonderful cook) has DONE IT!!!
We have adapted the recipe here for Zizzit's Flapjacks for coeliacs and gluten free diets. The method is pretty much the same, melt the sugar and syrup, stir in the dry ingredients etc, but the ingredient ratios and content has changed slightly as follows:-
Ingredients
Genius. Here's the proof....

We have adapted the recipe here for Zizzit's Flapjacks for coeliacs and gluten free diets. The method is pretty much the same, melt the sugar and syrup, stir in the dry ingredients etc, but the ingredient ratios and content has changed slightly as follows:-
Ingredients
- 6 oz demerera sugar
- 2 dessert spoons of golden syrup
- 8 oz margarine (we found half Pure marge and half Stork block work best but this is not essential)
- 12 oz gluten free oats
- 2 desert spoons gluten free flour
- Plus we added some raisins and chopped apricots - optional but delicious!
Genius. Here's the proof....

Saturday, 27 October 2012
"Constipation", Motility and Movicol
When you think of constipation, it is usually not only the inability to pass stool, but the passing of very hard, dry stool. This is indeed true constipation, but the term is frequently used to include all conditions where someone is unable to poo. Constipation is a very common problem for children and most of the time constipation does indeed mean passing hard stools, with difficulty, less frequently than normal. Unfortunately heading to a GP and explaining that your child is constipated without any details can cause considerable unintended complications, with potentially inappropriate medication prescribed which can have long term unwanted effects. Gut motility is central to treatment and the term "constipation" can be very misleading.
"Overflow" (loose stool flowing around the trapped hard stool) is often seen early in treatment regimes for constipation, when it appears laxatives have cleared the bowel out, but unless they are continued for approximately the same length of time the person has been constipated the bowel does not clear fully and will not contract back to enable it to function properly. Regular soiling because of overflow is often mistaken for runny diarrhoea but may indicate that a child has bad constipation with impaction (a blockage of stools/faeces).
As well as classic constipation, where your child might be straining to pass infrequent hard, dry stool there is such a thing as "slow transit" constipation, and there is dysmotility. In slow transit constipation relatively normal stool is passed, with otherwise normal - but slow- motility. There may or may not be straining on defecation - I will come to that later. There is also a condition known as dysmotility, which is slightly different. Treatment differs for all three types, or at least should do for best outcome.
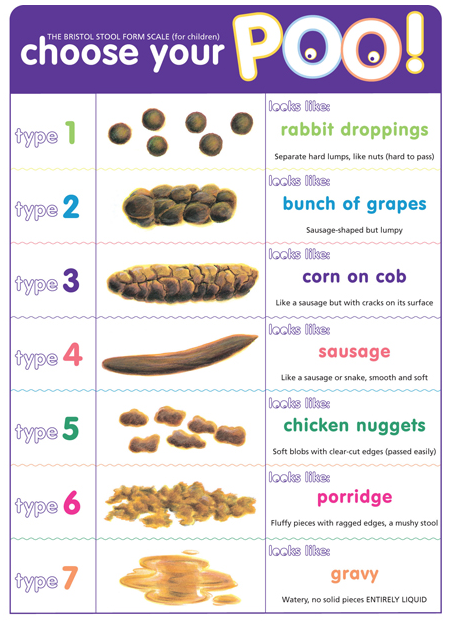
The Bristol Stool Chart for Children
Or you could make your own, like we did ;) Young children love toilet humour and humour is great for reducing tension and anxiety. Our own chart included "Jacket Potato Poo" and "Volcano Poo" amongst others, I will trade laughing over stress and anxiety any day.

The child who is presenting with rabbit dropping type stool or type 1 on the chart above would clearly benefit from more water in their stool. They may well not be drinking enough, and checking this is an excellent place to start. This type of constipation can also be a direct response to food/gut allergies but the latter is more likely to slow motility than affect the water content in the stool. That my personal observation though, I am happy to be corrected on that one!
 Movicol (or Miralax in the USA) is an osmotic laxative and a great drug for short term use in such cases (Type 1 stool) . It contains a plastic derivative that is used in disposable nappies (macrogol polyethylene glycol '3350) and just like the child who sits in a paddling pool with a nappy on, it swells with water. (try leaving a few sachets mixed overnight and see how it turns by morning.) This obviously DOES increase the water content..... but as you can see it will also increase stool volume.
Movicol (or Miralax in the USA) is an osmotic laxative and a great drug for short term use in such cases (Type 1 stool) . It contains a plastic derivative that is used in disposable nappies (macrogol polyethylene glycol '3350) and just like the child who sits in a paddling pool with a nappy on, it swells with water. (try leaving a few sachets mixed overnight and see how it turns by morning.) This obviously DOES increase the water content..... but as you can see it will also increase stool volume.
My big concern is that this drug is the routine first line medication for childhood constipation. Have you checked out the racks of frequently used prescription meds in Boots? Movicol is probably taking up at least a whole round shelf.... and every GP in the country seems to have a Movicol sponsored sticky notes pad. Great marketing..... but this drug is really not ideal if you are NOT dealing with classic constipation.
Slow transit constipation can actually result from chronic untreated/poorly or inadequately treated classic constipation. The bowel can become stretched as hard stool collects as bowel peristalsis struggles to move it along. In this scenario Movicol can be helpful to soften the stool but it will increase the stool volume in high doses, thus giving the bowel even more work to do at a time it is struggling. It is important to explain to your Dr about your child's stool consistency and normal pattern of passing stool, because if you are straying into the slow transit category Movicol use needs some caution. This is especially important in young children because there is a balancing act between being as gentle as possible, clearing the bowel effectively to avoid compounding the problem and ensuring you are not adding to the problem if motility is an issue.
Slow transit will often happen in an inflamed bowel, which cannot contract and relax as effectively as it might do despite stool being a normal consistency. I have explained how local allergic responses to food in the gut can impact on bowel motility here , in some there is a rapid response, if my youngest son ingested anything different as a baby his gut seemed to "switch off" whereas his twin sister would have a slower response, making it much more difficult to work out the trigger!
So the slow movement might be due to true constipation or it might be due to bowel inflammation (or other disease) but (and I had a recent discussion at GOS with our motility consultant about this) it is important to know as far as possible what you are treating, as high fibre/volume is not beneficial for a bowel which is struggling and when you are not dealing with a hard stool issue.
Dysmotility is slightly different. There are many different causes, and there are some excellent explanations here . It might involve a muscle problem or a nerve problem, and sadly the latter can happen as a direct result of chronic constipation. Muscle and nerve problems can be picked up in a test called Colonic Manometry, a very useful (although only available at GOS in this country at present) test to determine nerve and muscle function in the colon.
This is one of the problems my son is dealing with. As well as having slow transit due to inflammation (EGID) he has nerve damage in his colon as a result from years of having an inflamed and overloaded bowel. We were at the point where he needed the highest dose of the one of the strongest stimulant laxatives (sodium picosulphate) and was still only able to "go" approximately every 9-10 days, at which point the volume was so enormous that he would block the toilet frequently. It's not exactly rocket science when it comes to understanding how a dysmotile bowel or one with slower motility might struggle with large doses of fibre and or Movicol. The 8-12 sachets per day we had to give for over two years appeared to us to be contributing to, not helping the problem. After careful discussion with his doctors we decided to stop the Movicol..... and held our breath. He started going almost every day - still requiring the stimulant laxative - which was the most fabulous step forward. For us, Movicol was NOT the answer, and I wished I had understood the difference between transit problems and constipation a lot earlier. Our son now has an overly large (diameter) and far longer colon than usual, as a result of years of overloading it. This has caused nerve damage (which may heal over time) which is probably more severe than it would have been had we addressed the motility issues a lot earlier. My youngest son has EGID, is more complicated than "normal" but nonetheless it took far too long to determine the cause of his "constipation" and get him on appropriate medication.
Hirschsprung’s Disease is an uncommon motility problem marked by an absence of nerve cells in the walls of the rectum or colon. This condition is present at birth and can be hereditary. Without the necessary nerve cells, intestinal contractions cannot occur, and stool remains trapped in the large intestine, called obstruction. Not passing meconium, constipation, and vomiting are common symptoms. Treatment is primarily surgical, with the removal of affected tissue from the bowel.
Lastly there is the outlet obstruction type of constipation, where the stool consistency is not the issue, the motility is (initially) not the issue but the child has to strain and strain. This can be for different reasons. In the allergic gut, inflammation of the anal sphincter will inflame it and cause it to rest at a much higher pressure than normal. To pass stool, the sphincter pressure must be equalled from the other side, to cause it to relax. A sphincter at a very high pressure will require a large volume of stool (of whatever consistency) to be present to permit relaxation. The child will strain and strain and eventually pass a large volume of stool which might even be liquid but which cannot be passed until the volume creates sufficient pressure. Unfortunately this becomes a vicious circle, because the higher than normal volume needed eventually stretches the rectum and it becomes looser, so larger volume is needed to equalise the pressure and so on. Anorectal manometry is really useful for testing this potential problem. In the USA Botox has successfully been used to treat this problem but identifying the inflammatory triggers and treating the inflammation is the way forward.
Young children can also have functional constipation, such as withholding stool which should also be considered in a child of toilet training age. Whilst a behavioural issue it can cause longer term problems as you will work out from the info above. Stool collecting in any part of the colon over a long period is a potential problem and you should speak with your Health Visitor or GP.
Constipation of any sort will often impact on the entire GI tract. If one bit of the pipe functions less well, the rest will know about it. Reflux will be worse, abdominal pain is possible, reduced appetite with a feeling of fullness, and even retching and vomiting. This is very obvious in infants whose smaller bodies exhibit rapidly worsening reflux should they already suffer, and one reason why feed thickeners and so called "hungry baby" milks can make things so much worse. Digestion of solids and thickened milks takes longer, making the baby feel fuller for longer but allowing the stomach contents more time to reflux back. Hungry Baby Milk has no nutritional or calorific value over and above normal formula and is therefore only designed to make babies tummies feel fuller for longer presumably for the benefit of the parents, with potential problem resulting from delayed digestion for babies who already suffer with reflux.
If you are dealing with more severe motility problems there is an excellent article here in the Complex Child ezine.
As you can see, there is far more to "constipation" than needing to add water to the stool. It is important to have some idea of current stool consistency compared to your child's "normal" if consulting a doctor about it, and to initiate a discussion as to whether your child is going less frequently, having trouble passing the stool, and what that stool consistency is when coupled with those symptoms rather than merely reporting "constipation" and leaving the surgery with a box of Movicol sachets. There is a growing body of parents (and thankfully, doctors) who are concerned about the overuse and misuse of this apparently benign drug which I sincerely hope will avoid others going through some of the problems we have suffered, and still suffer today.
There is some excellent information here on constipation in children. Remember, Constipation can be very common in young children and occur for no obvious reason. (idiopathic) The information on this Blog is aimed at those parents managing children with underlying issues, such as allergic, inflammatory gut issues because that is the background I have, but in all cases of constipation in children careful note needs to be taken of the circumstances and symptoms.
DISCLAIMER - I am not a doctor, the information above I have ben told, read and learned over the years. The opinions are not only my own, but it must be stressed that this is a Blog not a medical document and whilst knowledge and opinion is useful you must follow the advice of your/your child's doctor. By all means discuss the above, I have carefully referenced the information but I am not medically trained.
"Overflow" (loose stool flowing around the trapped hard stool) is often seen early in treatment regimes for constipation, when it appears laxatives have cleared the bowel out, but unless they are continued for approximately the same length of time the person has been constipated the bowel does not clear fully and will not contract back to enable it to function properly. Regular soiling because of overflow is often mistaken for runny diarrhoea but may indicate that a child has bad constipation with impaction (a blockage of stools/faeces).
As well as classic constipation, where your child might be straining to pass infrequent hard, dry stool there is such a thing as "slow transit" constipation, and there is dysmotility. In slow transit constipation relatively normal stool is passed, with otherwise normal - but slow- motility. There may or may not be straining on defecation - I will come to that later. There is also a condition known as dysmotility, which is slightly different. Treatment differs for all three types, or at least should do for best outcome.
The Bristol Stool Chart for Children
Or you could make your own, like we did ;) Young children love toilet humour and humour is great for reducing tension and anxiety. Our own chart included "Jacket Potato Poo" and "Volcano Poo" amongst others, I will trade laughing over stress and anxiety any day.
 Movicol (or Miralax in the USA) is an osmotic laxative and a great drug for short term use in such cases (Type 1 stool) . It contains a plastic derivative that is used in disposable nappies (macrogol polyethylene glycol '3350) and just like the child who sits in a paddling pool with a nappy on, it swells with water. (try leaving a few sachets mixed overnight and see how it turns by morning.) This obviously DOES increase the water content..... but as you can see it will also increase stool volume.
Movicol (or Miralax in the USA) is an osmotic laxative and a great drug for short term use in such cases (Type 1 stool) . It contains a plastic derivative that is used in disposable nappies (macrogol polyethylene glycol '3350) and just like the child who sits in a paddling pool with a nappy on, it swells with water. (try leaving a few sachets mixed overnight and see how it turns by morning.) This obviously DOES increase the water content..... but as you can see it will also increase stool volume.My big concern is that this drug is the routine first line medication for childhood constipation. Have you checked out the racks of frequently used prescription meds in Boots? Movicol is probably taking up at least a whole round shelf.... and every GP in the country seems to have a Movicol sponsored sticky notes pad. Great marketing..... but this drug is really not ideal if you are NOT dealing with classic constipation.
Slow transit constipation can actually result from chronic untreated/poorly or inadequately treated classic constipation. The bowel can become stretched as hard stool collects as bowel peristalsis struggles to move it along. In this scenario Movicol can be helpful to soften the stool but it will increase the stool volume in high doses, thus giving the bowel even more work to do at a time it is struggling. It is important to explain to your Dr about your child's stool consistency and normal pattern of passing stool, because if you are straying into the slow transit category Movicol use needs some caution. This is especially important in young children because there is a balancing act between being as gentle as possible, clearing the bowel effectively to avoid compounding the problem and ensuring you are not adding to the problem if motility is an issue.
Slow transit will often happen in an inflamed bowel, which cannot contract and relax as effectively as it might do despite stool being a normal consistency. I have explained how local allergic responses to food in the gut can impact on bowel motility here , in some there is a rapid response, if my youngest son ingested anything different as a baby his gut seemed to "switch off" whereas his twin sister would have a slower response, making it much more difficult to work out the trigger!
So the slow movement might be due to true constipation or it might be due to bowel inflammation (or other disease) but (and I had a recent discussion at GOS with our motility consultant about this) it is important to know as far as possible what you are treating, as high fibre/volume is not beneficial for a bowel which is struggling and when you are not dealing with a hard stool issue.
Dysmotility is slightly different. There are many different causes, and there are some excellent explanations here . It might involve a muscle problem or a nerve problem, and sadly the latter can happen as a direct result of chronic constipation. Muscle and nerve problems can be picked up in a test called Colonic Manometry, a very useful (although only available at GOS in this country at present) test to determine nerve and muscle function in the colon.
This is one of the problems my son is dealing with. As well as having slow transit due to inflammation (EGID) he has nerve damage in his colon as a result from years of having an inflamed and overloaded bowel. We were at the point where he needed the highest dose of the one of the strongest stimulant laxatives (sodium picosulphate) and was still only able to "go" approximately every 9-10 days, at which point the volume was so enormous that he would block the toilet frequently. It's not exactly rocket science when it comes to understanding how a dysmotile bowel or one with slower motility might struggle with large doses of fibre and or Movicol. The 8-12 sachets per day we had to give for over two years appeared to us to be contributing to, not helping the problem. After careful discussion with his doctors we decided to stop the Movicol..... and held our breath. He started going almost every day - still requiring the stimulant laxative - which was the most fabulous step forward. For us, Movicol was NOT the answer, and I wished I had understood the difference between transit problems and constipation a lot earlier. Our son now has an overly large (diameter) and far longer colon than usual, as a result of years of overloading it. This has caused nerve damage (which may heal over time) which is probably more severe than it would have been had we addressed the motility issues a lot earlier. My youngest son has EGID, is more complicated than "normal" but nonetheless it took far too long to determine the cause of his "constipation" and get him on appropriate medication.
Hirschsprung’s Disease is an uncommon motility problem marked by an absence of nerve cells in the walls of the rectum or colon. This condition is present at birth and can be hereditary. Without the necessary nerve cells, intestinal contractions cannot occur, and stool remains trapped in the large intestine, called obstruction. Not passing meconium, constipation, and vomiting are common symptoms. Treatment is primarily surgical, with the removal of affected tissue from the bowel.
Lastly there is the outlet obstruction type of constipation, where the stool consistency is not the issue, the motility is (initially) not the issue but the child has to strain and strain. This can be for different reasons. In the allergic gut, inflammation of the anal sphincter will inflame it and cause it to rest at a much higher pressure than normal. To pass stool, the sphincter pressure must be equalled from the other side, to cause it to relax. A sphincter at a very high pressure will require a large volume of stool (of whatever consistency) to be present to permit relaxation. The child will strain and strain and eventually pass a large volume of stool which might even be liquid but which cannot be passed until the volume creates sufficient pressure. Unfortunately this becomes a vicious circle, because the higher than normal volume needed eventually stretches the rectum and it becomes looser, so larger volume is needed to equalise the pressure and so on. Anorectal manometry is really useful for testing this potential problem. In the USA Botox has successfully been used to treat this problem but identifying the inflammatory triggers and treating the inflammation is the way forward.
Young children can also have functional constipation, such as withholding stool which should also be considered in a child of toilet training age. Whilst a behavioural issue it can cause longer term problems as you will work out from the info above. Stool collecting in any part of the colon over a long period is a potential problem and you should speak with your Health Visitor or GP.
Constipation of any sort will often impact on the entire GI tract. If one bit of the pipe functions less well, the rest will know about it. Reflux will be worse, abdominal pain is possible, reduced appetite with a feeling of fullness, and even retching and vomiting. This is very obvious in infants whose smaller bodies exhibit rapidly worsening reflux should they already suffer, and one reason why feed thickeners and so called "hungry baby" milks can make things so much worse. Digestion of solids and thickened milks takes longer, making the baby feel fuller for longer but allowing the stomach contents more time to reflux back. Hungry Baby Milk has no nutritional or calorific value over and above normal formula and is therefore only designed to make babies tummies feel fuller for longer presumably for the benefit of the parents, with potential problem resulting from delayed digestion for babies who already suffer with reflux.
If you are dealing with more severe motility problems there is an excellent article here in the Complex Child ezine.
As you can see, there is far more to "constipation" than needing to add water to the stool. It is important to have some idea of current stool consistency compared to your child's "normal" if consulting a doctor about it, and to initiate a discussion as to whether your child is going less frequently, having trouble passing the stool, and what that stool consistency is when coupled with those symptoms rather than merely reporting "constipation" and leaving the surgery with a box of Movicol sachets. There is a growing body of parents (and thankfully, doctors) who are concerned about the overuse and misuse of this apparently benign drug which I sincerely hope will avoid others going through some of the problems we have suffered, and still suffer today.
There is some excellent information here on constipation in children. Remember, Constipation can be very common in young children and occur for no obvious reason. (idiopathic) The information on this Blog is aimed at those parents managing children with underlying issues, such as allergic, inflammatory gut issues because that is the background I have, but in all cases of constipation in children careful note needs to be taken of the circumstances and symptoms.
DISCLAIMER - I am not a doctor, the information above I have ben told, read and learned over the years. The opinions are not only my own, but it must be stressed that this is a Blog not a medical document and whilst knowledge and opinion is useful you must follow the advice of your/your child's doctor. By all means discuss the above, I have carefully referenced the information but I am not medically trained.
Thursday, 25 October 2012
All about Allergies, immunity and Autoimmune Conditions
When most of us think of the word "allergy" we are thinking of a systemic immune response, or at least an immediate and visible reaction. For myself as a child, allergies meant allergic rhinitis - streaming eyes, runny nose, and atopic reactions (rashes, usually itchy) to almost everything it seemed. My bedroom floor was regularly hoovered, as were the curtains and the bedding was washed every few days. My teddy lived in the freezer during the day for some time too to help eradicate the house dust mites I was so allergic to. I was on Beconase inhalers for years and we probably should have taken out shares in Piriton... However there are different kinds of allergic responses.
IgE MEDIATED RESPONSES
The above are all IgE mediated responses. True allergies, and allergies you can test for. IgE is an immunoglobulin. An immunoglobulin is "any of a class of proteins present in the serum and cells of the immune system, that function as antibodies". There are five subclasses of immunoglobulins, explained here far better than I could. DO read that link, it's the single best source I have found for non medics to explain your immune system and how it is classified.
IgE responses can be tested for - in Skin Prick Tests, and in RAST blood tests. The former have to be properly done to be accurate and reliable - we spent two years carting around an epipen for our second son who was allegedly allergic to peanuts - only to be retested a couple of years later (properly) and be told this was in fact rubbish. (Whilst some allergies can be outgrown, this is almost never the case with an IgE reaction to peanuts.) RAST blood tests are interesting, because they cannot in fact measure the severity of the reaction, the higher the number the higher the exposure rather than severity of response, so an older person would be expected to have a higher count.
NON IgE MEDIATED RESPONSES
You may think that a non IgE response would have to be what is termed an intolerance, but you would be wrong- along with an alarming number of health professionals I have encountered! An intolerance does not involve the immune system at all. A non IgE allergy is also known as a Type IV sensitivity, or cell mediated response. It is a local reaction and is rarely possible to test for. Gut allergies are delayed hypersensitivities, which is why food allergies are so traumatic and difficult to manage, requiring strict exclusion diets to determine responses to possible triggers. Imagine an eczema reaction in the gut - it's a localised response to an allergen (or a false allergen which the body responds inappropriately to) and causes a localised problem - no anaphylaxis, no outside response (although IgE responses are often present in addition in those with gut allergies) and is very difficult to diagnose.
Gut allergies are always responses to proteins, protein molecules are those the immune system responds to. Problems with carbohydrates/sugars such as lactose intolerance are not (as far as I know!) allergies.
GUT INFLAMMATION
Now imagine that patch of inflamed, irritated gastrointestinal tract - if your skin has a patch of eczema it is less supple, less flexible, cannot function at its best. Gut tissue is the same - it cannot function as well as it becomes inflamed. Inflammation ANYWHERE in the GI tract can cause symptoms anywhere else along its length. So, you can have reflux (which is only ever a symptom, be it from food allergy, obesity, muscle disease, ligament laxity, developmental delay etc) constipation, vomiting, diarrhoea, trapped wind, acute pain, chronic pain, bloating, wind - all from gut inflammation due to a localised allergic response. All too often I hear of children and adults with reflux symptoms, who have an upper endoscopy ("scope" where a camera is used to look down your throat as far as your stomach, and sometimes down to the small intestine below but only a small way down.) and a ph study which is negative and they are told there is no inflammation, no problem. It's happened to us too, my daughter was fobbed off for years until someone bothered to look lower and found inflammation and ulceration, causing the reflux further up. Bowel inflammation can, and does cause reflux. There are often other clues but sometimes it is that simple.
APPROPRIATE CARE
What is so concerning is the difficulty so many parents are having in getting appropriate care for children with clear reactions to food. Any parent with a child suffering from food allergies will tell you how their child reacts - yet if skin prick tests and RAST tests are negative many doctors come to the conclusion there cannot possibly be an immune response. Some doctors prescribe patch testing, which does indeed show delayed responses, but only on the skin. If it is only your gut tissues which is reacting, they are not going to be particularly helpful.
Another useful test is an serum IgA blood test. Immunoglobulin A is the major antibody found in the membranes of the respiratory and gastrointestinal tract. The second most common immunoglobulin in the human body, IgA can also be found in tears, saliva, mucus, and colostrums. IgA is one of the most important immonoglobulins in local immunity. Interestingly those with gut allergies often have low IgA levels, and in those who outgrow their gut allergies their IgA levels often rise approximately 6 months before such improvement become obvious when closely monitored. This is another reason why the antibiotic Azithromycin is so successful as an anti inflammatory agent in the gut, because of its role in the absence of IgA.
REFLUX and GUT INFLAMMATION
There is a huge surge in babies with reflux in the West, which is often due to gut allergies such as Cows Milk Protein allergy or reactions to other food proteins. It is often outgrown by the age of one but in those whom it persists into childhood underlying causes need to be investigated - any paediatrician should tell you that. The gold standard test for reflux used to be a ph study, measuring the ph at the top of the stomach. However, reflux caused by bowel inflammation is unlikely to be acidic unless the stomach contents at that time are acidic! Reflux caused by bowel inflammation is more likely to be alkaline, and shows up best using an impedance study or pressure test, used in conjunction with a ph probe. Gut inflammation will reduce gut functionality and therefore cause pressure changes along the GI tract.
No one is exactly sure why there is almost an epidemic of gut inflammation in the West. Many will tell you it is the overuse of antibiotics, the increasing prevalence of GM foods, over production , pesticides, chemicals etc but the truth is we just don't know. One thing is certain though that gut allergies are on the rise. In America there has been a surge in the number of diagnosed Coeliac Disease cases - interestingly Coeliac is another delayed hypersensitivity, as is Chrohn's Disease. Eosinophilic Disease is also thought to fit into this category which makes it so very difficult to treat and manage.
FOOD ALLERGIES AND BEHAVIOUR
Until quite recently there was little understanding of the way gut allergies worked. Recent research at Great Ormond Street has shown how neurotransmitters in the gut sit next to mast cells which are responsible for these local gut reactions. As these mast cells degranulate they release huge quantities of toxins which cause a local pain feedback cycle. They are also soaked up by the neurotransmitters and enter the central nervous system. This is thought to be how food allergic reactions cause the behavioural issues we often see in children with food allergies and could also explain why the casein and gluten free diet for Autism might just work for some children, who in fact display ASD type behaviours due to delayed gut hypersensitivities.
VACCINATIONS
Local gut reactions also cause an increase in histamine levels which make the gut wall more permeable. Anyone heard of Leaky Gut Syndrome? Something I thought highly "alternative" and improbable until I was immersed unwillingly into the world of gut allergies. What is more concerning is recent GOS research which is supporting the theory that the blood brain barrier is permeable (as is the gut) when local immune activity is present. Teething can also precipitate this permeability by raising histamine levels. There is in fact current speculation as to whether a highly allergic child - whether IgE or non IgE - and/or one who is actively teething should have their vaccines postponed/delayed. This is similar to the theory postulated by Andrew Wakefield, whose totally flawed study left him hung out to dry but which buried the real message that timing is actually important with vaccination and that the links between the gut, Autism and vaccination might well have more to do with histamine and gut permeability than multiple vaccination programmes.
AUTOIMMUNE DISEASES
Lastly what i find particularly interesting coming from an EGID perspective is that several Autoimmune diseases are also Type IV hypersensitivites. Hashimoto's Thyroid Disease (which I suffer from) Diabetes Type 1, Arthritis... all the same type of reaction by the body. There are extremely strong links between gut allergies, immune profiles and autoimmune diseases. My children also have low IgM and IgG levels - again, common in those with autoimmune disease, but also caused by gut inflammatory conditions!
So despite being non-IgE, impossible to test for allergies, the immune profile of these localised, delayed hypersensitivities is perhaps more profound than the more obvious, recognisable IgE responses we are all more familiar with. I think it's about time the medical profession sat up and took notice of the autoimmune time bomb in the West and the surge in gut allergies - REAL food allergies so many people (and particularly so many children) suffer from ARE relevant, and health professionals in the twenty first century have a responsibility to take them very seriously indeed.
DISCLAIMER - I am not a doctor, the information above I have ben told, read and learned over the years. The opinions are not only my own, but it must be stressed that this is a Blog not a medical document and whilst knowledge and opinion is useful you must follow the advice of your/your child's doctor. By all means discuss the above, I have carefully referenced the information but I am not medically trained. I support and endorse vaccination programmes - having children with reduced immunity I know the importance of herd immunity and prevention of disease. I always endeavour to research issues affecting our family however and take each intervention as an individual case.
IgE MEDIATED RESPONSES
The above are all IgE mediated responses. True allergies, and allergies you can test for. IgE is an immunoglobulin. An immunoglobulin is "any of a class of proteins present in the serum and cells of the immune system, that function as antibodies". There are five subclasses of immunoglobulins, explained here far better than I could. DO read that link, it's the single best source I have found for non medics to explain your immune system and how it is classified.
IgE responses can be tested for - in Skin Prick Tests, and in RAST blood tests. The former have to be properly done to be accurate and reliable - we spent two years carting around an epipen for our second son who was allegedly allergic to peanuts - only to be retested a couple of years later (properly) and be told this was in fact rubbish. (Whilst some allergies can be outgrown, this is almost never the case with an IgE reaction to peanuts.) RAST blood tests are interesting, because they cannot in fact measure the severity of the reaction, the higher the number the higher the exposure rather than severity of response, so an older person would be expected to have a higher count.
NON IgE MEDIATED RESPONSES
You may think that a non IgE response would have to be what is termed an intolerance, but you would be wrong- along with an alarming number of health professionals I have encountered! An intolerance does not involve the immune system at all. A non IgE allergy is also known as a Type IV sensitivity, or cell mediated response. It is a local reaction and is rarely possible to test for. Gut allergies are delayed hypersensitivities, which is why food allergies are so traumatic and difficult to manage, requiring strict exclusion diets to determine responses to possible triggers. Imagine an eczema reaction in the gut - it's a localised response to an allergen (or a false allergen which the body responds inappropriately to) and causes a localised problem - no anaphylaxis, no outside response (although IgE responses are often present in addition in those with gut allergies) and is very difficult to diagnose.
Gut allergies are always responses to proteins, protein molecules are those the immune system responds to. Problems with carbohydrates/sugars such as lactose intolerance are not (as far as I know!) allergies.
GUT INFLAMMATION
Now imagine that patch of inflamed, irritated gastrointestinal tract - if your skin has a patch of eczema it is less supple, less flexible, cannot function at its best. Gut tissue is the same - it cannot function as well as it becomes inflamed. Inflammation ANYWHERE in the GI tract can cause symptoms anywhere else along its length. So, you can have reflux (which is only ever a symptom, be it from food allergy, obesity, muscle disease, ligament laxity, developmental delay etc) constipation, vomiting, diarrhoea, trapped wind, acute pain, chronic pain, bloating, wind - all from gut inflammation due to a localised allergic response. All too often I hear of children and adults with reflux symptoms, who have an upper endoscopy ("scope" where a camera is used to look down your throat as far as your stomach, and sometimes down to the small intestine below but only a small way down.) and a ph study which is negative and they are told there is no inflammation, no problem. It's happened to us too, my daughter was fobbed off for years until someone bothered to look lower and found inflammation and ulceration, causing the reflux further up. Bowel inflammation can, and does cause reflux. There are often other clues but sometimes it is that simple.
APPROPRIATE CARE
What is so concerning is the difficulty so many parents are having in getting appropriate care for children with clear reactions to food. Any parent with a child suffering from food allergies will tell you how their child reacts - yet if skin prick tests and RAST tests are negative many doctors come to the conclusion there cannot possibly be an immune response. Some doctors prescribe patch testing, which does indeed show delayed responses, but only on the skin. If it is only your gut tissues which is reacting, they are not going to be particularly helpful.
Another useful test is an serum IgA blood test. Immunoglobulin A is the major antibody found in the membranes of the respiratory and gastrointestinal tract. The second most common immunoglobulin in the human body, IgA can also be found in tears, saliva, mucus, and colostrums. IgA is one of the most important immonoglobulins in local immunity. Interestingly those with gut allergies often have low IgA levels, and in those who outgrow their gut allergies their IgA levels often rise approximately 6 months before such improvement become obvious when closely monitored. This is another reason why the antibiotic Azithromycin is so successful as an anti inflammatory agent in the gut, because of its role in the absence of IgA.
REFLUX and GUT INFLAMMATION
There is a huge surge in babies with reflux in the West, which is often due to gut allergies such as Cows Milk Protein allergy or reactions to other food proteins. It is often outgrown by the age of one but in those whom it persists into childhood underlying causes need to be investigated - any paediatrician should tell you that. The gold standard test for reflux used to be a ph study, measuring the ph at the top of the stomach. However, reflux caused by bowel inflammation is unlikely to be acidic unless the stomach contents at that time are acidic! Reflux caused by bowel inflammation is more likely to be alkaline, and shows up best using an impedance study or pressure test, used in conjunction with a ph probe. Gut inflammation will reduce gut functionality and therefore cause pressure changes along the GI tract.
No one is exactly sure why there is almost an epidemic of gut inflammation in the West. Many will tell you it is the overuse of antibiotics, the increasing prevalence of GM foods, over production , pesticides, chemicals etc but the truth is we just don't know. One thing is certain though that gut allergies are on the rise. In America there has been a surge in the number of diagnosed Coeliac Disease cases - interestingly Coeliac is another delayed hypersensitivity, as is Chrohn's Disease. Eosinophilic Disease is also thought to fit into this category which makes it so very difficult to treat and manage.
FOOD ALLERGIES AND BEHAVIOUR
Until quite recently there was little understanding of the way gut allergies worked. Recent research at Great Ormond Street has shown how neurotransmitters in the gut sit next to mast cells which are responsible for these local gut reactions. As these mast cells degranulate they release huge quantities of toxins which cause a local pain feedback cycle. They are also soaked up by the neurotransmitters and enter the central nervous system. This is thought to be how food allergic reactions cause the behavioural issues we often see in children with food allergies and could also explain why the casein and gluten free diet for Autism might just work for some children, who in fact display ASD type behaviours due to delayed gut hypersensitivities.
VACCINATIONS
Local gut reactions also cause an increase in histamine levels which make the gut wall more permeable. Anyone heard of Leaky Gut Syndrome? Something I thought highly "alternative" and improbable until I was immersed unwillingly into the world of gut allergies. What is more concerning is recent GOS research which is supporting the theory that the blood brain barrier is permeable (as is the gut) when local immune activity is present. Teething can also precipitate this permeability by raising histamine levels. There is in fact current speculation as to whether a highly allergic child - whether IgE or non IgE - and/or one who is actively teething should have their vaccines postponed/delayed. This is similar to the theory postulated by Andrew Wakefield, whose totally flawed study left him hung out to dry but which buried the real message that timing is actually important with vaccination and that the links between the gut, Autism and vaccination might well have more to do with histamine and gut permeability than multiple vaccination programmes.
AUTOIMMUNE DISEASES
Lastly what i find particularly interesting coming from an EGID perspective is that several Autoimmune diseases are also Type IV hypersensitivites. Hashimoto's Thyroid Disease (which I suffer from) Diabetes Type 1, Arthritis... all the same type of reaction by the body. There are extremely strong links between gut allergies, immune profiles and autoimmune diseases. My children also have low IgM and IgG levels - again, common in those with autoimmune disease, but also caused by gut inflammatory conditions!
So despite being non-IgE, impossible to test for allergies, the immune profile of these localised, delayed hypersensitivities is perhaps more profound than the more obvious, recognisable IgE responses we are all more familiar with. I think it's about time the medical profession sat up and took notice of the autoimmune time bomb in the West and the surge in gut allergies - REAL food allergies so many people (and particularly so many children) suffer from ARE relevant, and health professionals in the twenty first century have a responsibility to take them very seriously indeed.
DISCLAIMER - I am not a doctor, the information above I have ben told, read and learned over the years. The opinions are not only my own, but it must be stressed that this is a Blog not a medical document and whilst knowledge and opinion is useful you must follow the advice of your/your child's doctor. By all means discuss the above, I have carefully referenced the information but I am not medically trained. I support and endorse vaccination programmes - having children with reduced immunity I know the importance of herd immunity and prevention of disease. I always endeavour to research issues affecting our family however and take each intervention as an individual case.
MEWS free bread on prescription
 Some GP practices will prescribe gluten free products for those on medical exclusion diets other than exclusively for coeliac disease patients. Because EGID is a similar process to coeliac disease (only triggered by many foods and environmental allergens rather than just gluten) and can be diagnosed conclusively by biopsy in most our PCT have prescribed gluten free products for the twins for a couple of years.
Some GP practices will prescribe gluten free products for those on medical exclusion diets other than exclusively for coeliac disease patients. Because EGID is a similar process to coeliac disease (only triggered by many foods and environmental allergens rather than just gluten) and can be diagnosed conclusively by biopsy in most our PCT have prescribed gluten free products for the twins for a couple of years.Recently however we have had to reduce our egg intake, AND NHS Suffolk have dramatically reduced their prescribable products list and no longer offer the full Coeliac Society list they used to support. This left us high and dry since many of their currently endorsed products contain milk and or soya. None of the pastas now available are suitable, all contain soya flour for example.
We had to do the research ourselves and discovered Juvela Harvest White was the best solution. It's an excellent MEWS free flour mix which I prefer to make in to rolls, the loaves are ok when fresh but not great afterwards. Rolls need freezing if not being eaten within 24 hours and need a little freshening up before eating after defrosting. This does mean they don't work for school packed lunches unless fresh, but I have now got it down to a fine art and make half a box every other day. Labour intensive... but it works and both twins will eat them!
Sunday, 23 September 2012
Coconut Flour
 Desperately trying to find new gluten free options I discovered Tiana Coconut Flour in our local Holland and Barrett store and had to try it.
Desperately trying to find new gluten free options I discovered Tiana Coconut Flour in our local Holland and Barrett store and had to try it.It is high in fibre so might not suit all, but it is filling and easy to cook with (apparently!) It says you do need a wetter mixture if partially substituting in regular recipes, so do read the Tiana site first.
My first attempt at baking was not that good, despite making the effort to read the tips on the Tiana site (Recipes & Diets -> Baking with Coconut flour --> tips ) and trawling the web for a suitable conversion chart from imperial cups to imperial oz or even metric grams.
But I have now found a fantastic conversion chart (here) which works beautifully!
Today I retried the recipe I first attempted, (a basic coconut biscuit recipe) but today it worked a treat.
Baking with Tiana is not cake baking but batter baking, it relies on eggs so I would not like to make assumptions about it working with egg alternatives, although I might try the Vegg with it.
I used the recipe below.
You DO need to allow the batter to stand for 5-10 minutes to thicken up. I used a Pampered Chef scoop which is a little like a melon baller - I don't really rate Pampered Chef but this tool WORKS!! (It's fab for little cupcakes and biscuits.) I then flattened the balls a tiny bit with the back of a spoon, baked at 190 C for 15 mins and IT WORKED!!! These are rather moreish... be warned! For children who are deprived of so many regular tastes and textures this is a fab find, and has enhance our repertoire considerably.
Coconut Almond Cookies
1/2 cup Tiana coconut flour
1/2 cup ground almonds
1/2 cup butter (I used "Pure" Sunflower)
1 cup sugar (I used caster)
1/4 teaspoon salt
4 eggs
3/4 tsp almond extract (optional)

Unlike a cake, the instructions do not tell you to beat the sugar and butter together, just make sure the butter/marge is room temperature, and mix it with the sugar, eggs and salt, plus almond extract if you are using it. Stir in the flour and ground almonds. Let the batter rest for 5-10 minutes. Drop on a baking sheet in small spoon sized balls. Bake for 15 mins at 190 C until browned.

(NB the Tiana site suggests toasted almonds instead of ground almonds, and 1 1/ cups of grated coconut as well. I took advantage of the ground almond consistency as I didn't have any coconut.)
“This post is an entry into the Foodies100/Schwartz Flavour of Together challenge.” Do you have a revolutionary flavour or ingredient which is particularly significant, evocative of times past or which adds something new to your alimentary life? Check out the Schwartz website to share your #FlavourStories !

Saturday, 22 September 2012
Egg alternatives/substitutes
At the time this post was written, I was rather lax in investigating egg alternatives as we were not egg free. All that changed about six years ago and my daughter and I are now experienced #eggfree bakers! There is another post here with lots of easy alternatives. Free from baking should always be a little wetter than regular batters and mixes, it takes a bit of getting used to. It can be frustrating and the ingredients are not cheap (eg chia seeds) but the results can be really good - it's worth persevering. Free from sweet items in the supermarkets are all too often full of cheap fillers and a great deal of sugar (to hide the lack of flavour due to removal of proteins) so if you can possible bake your own, it's incredibly worthwhile.
A friend posted this chart elsewhere, it is an invaluable resource for those trying to exclude egg in cooking so I thought I would share it here.

A friend posted this chart elsewhere, it is an invaluable resource for those trying to exclude egg in cooking so I thought I would share it here.

Monday, 10 September 2012
Packed lunches
I've been really struggling to make interesting MEWS free packed lunches for my twins. Few egg free breads are palatable if they cannot be freshened up in the microwave which is obviously not possible at nursery/school. My two (currently!) seem to like Falafel, which is quick and easy to make. The Orgran one is OK, the Hale and Hearty mix is less crunchy (smoother consistency) but sloppier if mixed as instructed and more difficult to make round balls to fry. These also seemed to dry out faster in the fridge. Our favourite is the one our Co-Op sells, the "Just" range.
(If you are ok with corn Barkat make one with few ingredients but I have not tried this mix myself.)
 So, today's cooking session was devoted to making Falafel and finding something to add with it. I have some tiny tupperware boxes I put sauces and dips in, so one twin has mayonnaise and the other ketchup to dunk these in tomorrow.
So, today's cooking session was devoted to making Falafel and finding something to add with it. I have some tiny tupperware boxes I put sauces and dips in, so one twin has mayonnaise and the other ketchup to dunk these in tomorrow.
Given the bread problem mentioned above, I have been taking the advice on a friend on how to perfect rolls made with the Juvela Harvest White bread mix. I had no END of trouble getting the correct mix prescribed, this is the only one Suffolk PCT will sanction for those who are gluten free which is also dairy and soya free. DO read labels and check any bread mixes if you are lucky enough to receive gluten free prescription food. Mixes frequently contain other foods many children are excluding as they tend to cater for the gluten free category only.
 This bread mix works particularly well as rolls, and you can now buy dairy AND soya free cheese from a couple of sources. I used this to create a cheezy topping on some rolls today, you could make cheese twists or even add some to the mix and make cheese rolls! I am indebted to Rebecca for these fabulous tried and tested suggestions.
This bread mix works particularly well as rolls, and you can now buy dairy AND soya free cheese from a couple of sources. I used this to create a cheezy topping on some rolls today, you could make cheese twists or even add some to the mix and make cheese rolls! I am indebted to Rebecca for these fabulous tried and tested suggestions.
Holland and Barrett on the high street stock Redwood Cheezly Soy free which is easy to source, but our favourite is the Vegusto cheese! BE WARNED though, their cheese contain nut protein, and NOT ALL their products are free from major allergens. They are intended as Vegan cheese products. The Melty is fab, often out of stock...... and the hard cheese we like is the No Moo Aromatic Cheddar. Strong tasting, but my daughter likes strong flavours! Her twin won't touch ANY cheese substitutes :S
(If you are ok with corn Barkat make one with few ingredients but I have not tried this mix myself.)

Given the bread problem mentioned above, I have been taking the advice on a friend on how to perfect rolls made with the Juvela Harvest White bread mix. I had no END of trouble getting the correct mix prescribed, this is the only one Suffolk PCT will sanction for those who are gluten free which is also dairy and soya free. DO read labels and check any bread mixes if you are lucky enough to receive gluten free prescription food. Mixes frequently contain other foods many children are excluding as they tend to cater for the gluten free category only.
 This bread mix works particularly well as rolls, and you can now buy dairy AND soya free cheese from a couple of sources. I used this to create a cheezy topping on some rolls today, you could make cheese twists or even add some to the mix and make cheese rolls! I am indebted to Rebecca for these fabulous tried and tested suggestions.
This bread mix works particularly well as rolls, and you can now buy dairy AND soya free cheese from a couple of sources. I used this to create a cheezy topping on some rolls today, you could make cheese twists or even add some to the mix and make cheese rolls! I am indebted to Rebecca for these fabulous tried and tested suggestions.Holland and Barrett on the high street stock Redwood Cheezly Soy free which is easy to source, but our favourite is the Vegusto cheese! BE WARNED though, their cheese contain nut protein, and NOT ALL their products are free from major allergens. They are intended as Vegan cheese products. The Melty is fab, often out of stock...... and the hard cheese we like is the No Moo Aromatic Cheddar. Strong tasting, but my daughter likes strong flavours! Her twin won't touch ANY cheese substitutes :S
So here we have some with and some without cheese. I have eaten these too, they are very palatable but do take some practice getting the method just right.
Please do email me any of your lunch box ideas to help others!
Please do email me any of your lunch box ideas to help others!
Thursday, 3 May 2012
Raising Awareness for Eosinophilic Awareness Week
Healthy Eating - What it means for us
The third week in May is Eosinophilic Awareness Week. Help raise awareness of food allergies, and their impact on young lives by considering sharing this child-friendly information with your child's school:-
"There are different types of food allergies. We have Eosinophilic Disease, when the body gets confused and thinks some foods are like germs and need attacking. The problem is this attack can end up hurting your body too! Eating those foods make your throat, tummy or bowel red and sore and stops them working properly. If you are not careful then things we all take for granted like eating, swallowing and digesting food don’t happen properly. Going to the toilet can be painful, take a long time and be really difficult.
Like any other food allergy you must stop eating the food your body is reacting to. Some people react in a quick, dangerous way to foods. This can be life threatening. Others react more slowly but the long term effect can be very serious. All our bodies like to be cared for, letting them get red, sore and swollen for long periods of time can damage them. Our bodies work best when they are properly cared for. We all try and look after our teeth by not eating too many sweets! If you have a food allergy you look after your body by avoiding those foods your body reacts to. Sometimes that means you cannot eat foods which have important things in them for growing. That can mean you need to find those important things in other foods, or in a special formula drink, and take medicines to keep healthy.
We all know someone who cannot eat nuts, or eggs, maybe both. Imagine not being able to eat anything made from milk, AND nothing made from wheat, gluten - which includes oats - OR soya. It’s hard. Getting enough energy is really important - we use a lot of it in school! So sometimes food you might think is less healthy is just right for us! Healthy Eating is really important. It is about looking after your body. But most of all it is about eating in a way to take care of your own body in the best way possible for you."

The third week in May is Eosinophilic Awareness Week. Help raise awareness of food allergies, and their impact on young lives by considering sharing this child-friendly information with your child's school:-
"There are different types of food allergies. We have Eosinophilic Disease, when the body gets confused and thinks some foods are like germs and need attacking. The problem is this attack can end up hurting your body too! Eating those foods make your throat, tummy or bowel red and sore and stops them working properly. If you are not careful then things we all take for granted like eating, swallowing and digesting food don’t happen properly. Going to the toilet can be painful, take a long time and be really difficult.
Like any other food allergy you must stop eating the food your body is reacting to. Some people react in a quick, dangerous way to foods. This can be life threatening. Others react more slowly but the long term effect can be very serious. All our bodies like to be cared for, letting them get red, sore and swollen for long periods of time can damage them. Our bodies work best when they are properly cared for. We all try and look after our teeth by not eating too many sweets! If you have a food allergy you look after your body by avoiding those foods your body reacts to. Sometimes that means you cannot eat foods which have important things in them for growing. That can mean you need to find those important things in other foods, or in a special formula drink, and take medicines to keep healthy.
We all know someone who cannot eat nuts, or eggs, maybe both. Imagine not being able to eat anything made from milk, AND nothing made from wheat, gluten - which includes oats - OR soya. It’s hard. Getting enough energy is really important - we use a lot of it in school! So sometimes food you might think is less healthy is just right for us! Healthy Eating is really important. It is about looking after your body. But most of all it is about eating in a way to take care of your own body in the best way possible for you."

Sunday, 29 April 2012
Healthy Eating?
This was published as a Blog post here and on my personal Blog, but it's such a hot topic I have made it a permanent page - at least for now!

Today K and A's school included in their weekly "newspaper" an editorial on "Healthy Eating", asking parents to support the school's two week drive to improve on an already ongoing campaign.
But just what IS Healthy Eating? The school in question have twice termly cake sales, and hands out sweets in birthday assembly, which hardly fits the "Healthy Eating" criteria that the school is so keen to promote? But actually I have more support for cake sales than you might think. The key to good health is usually a balance in all things, cakes have their place in our children's diets as much as fruit, more so if you speak to a dentist - many of whom deplore the plethora of dried fruit snacks which are the biggest culprits for causing cavities in young children today. On the subject of fruit generally the message is the same, balance is key:-
"It might seem counter intuitive to think that a food with lots of sugar is good for your teeth, but fresh fruit is good for your teeth when consumed as part of a balanced diet."
However frequency also matters, and the modern craze for snacking does no one's teeth, blood sugar or appetite any favours.
Given that my younger two are on such restricted diets their school's two snacks a day (which has to be fruit or cheese) means we probably hit 5-a-day by lunch time, so I am not going to lose any sleep about the odd free-from cake which their school very thoughtfully provides for those unable to buy the regular cakes at their charity sales. My bigger concern is the drive for low fat-high sugar foods, the demonising of animal fats and the rising importance of carbohydrates in society- and initiative endorsed by successive governments over the past couple of decades. The NHS' "Eatwell Plate" demonstrates clearly this change in focus, and the obesity surge and diabetes time bomb are evidence of how badly wrong politicians and health experts have been. The comments at the bottom of this NHS page do a far, far better job than I could of explaining how skewed our thinking has become about fats and carbohydrates. The processed food industry has been key in promoting grains and sugars, particularly fructose and sucrose with government support but many people are cottoning on slowly, with a surge in online writings trying to expose the myth that vegetable oils are good and animal fats are bad. Even schools are caught up in the effort to increase carbs and fruit and this frustrates me considerably.
My biggest issue with the "Healthy Eating" campaign though, be it at their school or elsewhere, is that I would really prefer my kids to eat for fuel and pleasure - social, sensory, satiety pleasures - and not think too much about it. I resent having to read every label, cook everything from scratch all the time and stress over their daily intake as it is, I try hard (and it IS hard) to ensure their lives are as normal as possible, that they don't feel too different and they don't miss out. But most of all, I would like for food and eating to be necessity not a focus, to take a back seat in life and just be something I as their mother need to consider. If we get through a day where the children have eaten when hungry, had their fill and run off back to more interesting activities then I have succeeded. A day spent thinking about every bite, each ingredient, its impact and value is a day wasted for a child, it is the responsibility of adults to feed their children appropriately and make it as mundane a process most of the time as filling the car with petrol. Of course food is to be enjoyed, but to make it a major or even the sole focus of a child's life for even a short period of time is as bad as ignoring natural appetite.
I have to say, I write none of this whilst wearing an imaginary halo, I fail miserably at this ideal many days and the children's extremely restricted diet makes it very, very difficult to achieve even our own version of normality. But my heart sank reading that newsletter column tonight, because all my efforts made on a daily basis will be shot down in flames in a misguided fortnight of demonising fats, pushing carbs, vegetable oils and fruit - but most of all in drawing attention to something which I would prefer my children not to have to think about. Add to that the fact that they will most likely be discrediting foods my twins rely on to keep them well and it's not going to be a positive experience I fear. I hope I'm wrong.

Wednesday, 28 March 2012
Chocolate and Pear Muffins!
Sound different? Unusual? They are delicious!
We were a little tired of the delicious Banana Muffins...
and I had rather too many squashy conference pears in my fridge... so decided to get inventive.
I peeled and cored four small pears. Chopped and microwaved them until cooked. Then substituted the bananas in this recipe for pears, and substituted 1 oz of the flour for 2 oz cocoa powder. (Pear is a little wetter than banana so needed more dry ingredients.)
I have also substituted apple and blackberries in the same way before, but strained the excess juice out first and added an ounce of oats to soak up the moisture. Not all of you can have oats I know (and I don't know if gluten free oats would work as well) but worth a try if you can!
Bake as before, and Voila!

We were a little tired of the delicious Banana Muffins...
I peeled and cored four small pears. Chopped and microwaved them until cooked. Then substituted the bananas in this recipe for pears, and substituted 1 oz of the flour for 2 oz cocoa powder. (Pear is a little wetter than banana so needed more dry ingredients.)
I have also substituted apple and blackberries in the same way before, but strained the excess juice out first and added an ounce of oats to soak up the moisture. Not all of you can have oats I know (and I don't know if gluten free oats would work as well) but worth a try if you can!

Thursday, 1 March 2012
Running for Gt Ormond Street Children's Charity!
He has always loved Athletics and currently runs with a local club, enjoying a very successful 2011/2012 season so far! Several members of our family suffer with Gastrointestinal Disease and associated conditions. Josh's youngest siblings are treated at Great Ormond Street Hospital and we as a family are incredibly grateful for the support and treatment we receive from there. The twins' Consultant has recently climbed Kilimanjaro to raise funds for new gastro research and treatment so Josh decided to do his bit! Climbing mountains was a bit ambitious, so instead he is running 5K in Suffolk on 13th May at Alton Water, in Suffolk.
Josh regularly runs between 2 and 7 K, competing several years above his age group. He too has suffered gastro issues as a young child and joint problems since and really hopes GOSH can help make a difference for others.
We and so many others would be incredibly grateful if you felt able to sponsor him, our JustGiving Page is here.
Thursday, 23 February 2012
Oven Baked Rissotto
Free from Dairy (IF THE CHEESE IS EXCLUDED) , Soya, Wheat, Gluten, Egg and Corn.
You need:
Instructions
You need:
- 250g smoked bacon chopped into small pieces
- 1 onion chopped
- 1oz Pure Sunflower or similar
- 10 oz Arborio rice
- 150g cherry tomatoes (I often replace this with 300g mushrooms)
- 700ml chicken stock
- 2 oz grated parmesan (leave out or substitute if dairy free)
Instructions
- Heat oven to 180 degrees
- Fry bacon pieces in casserole dish (dry fry) for 3-5 minutes until golden and crisp. Dish need to be able to go on hob.
- Stir in onion and butter and cook for 3-4 mins until soft
- Pour in rice and mix well until all rice is coated in juice from onions
- Pour in wine and cook until all liquid absorbed
- Add cherry tomatoes, hot stock and give quick stir
- Cover with lid, put in oven and cook for 18 mins stirring occasionally (I did it twice).
- Stir in parmesan and stir until melted
- Serve and sprinkle with extra parmesan
Subscribe to:
Comments (Atom)