When you think of constipation, it is usually not only the inability to pass stool, but the passing of very hard, dry stool. This is indeed true constipation, but the term is frequently used to include all conditions where someone is unable to poo. Constipation is a very common problem for children and most of the time constipation does indeed mean passing hard stools, with difficulty, less frequently than normal. Unfortunately heading to a GP and explaining that your child is constipated without any details can cause considerable unintended complications, with potentially inappropriate medication prescribed which can have long term unwanted effects. Gut motility is central to treatment and the term "constipation" can be very misleading.
"
Overflow" (loose stool flowing around the trapped hard stool) is often seen early in treatment regimes for constipation, when it appears laxatives have cleared the bowel out, but unless they are continued for approximately the same length of time the person has been constipated the bowel does not clear fully and will not contract back to enable it to function properly. Regular soiling because of overflow is often mistaken for runny diarrhoea but may indicate that a child has bad constipation with impaction (a blockage of stools/faeces).
As well as
classic constipation, where your child might be straining to pass infrequent hard, dry stool there is such a thing as "slow transit" constipation, and there is dysmotility. In slow transit constipation relatively normal stool is passed, with otherwise normal - but slow- motility. There may or may not be straining on defecation - I will come to that later. There is also a condition known as dysmotility, which is slightly different. Treatment differs for all three types, or at least should do for best outcome.
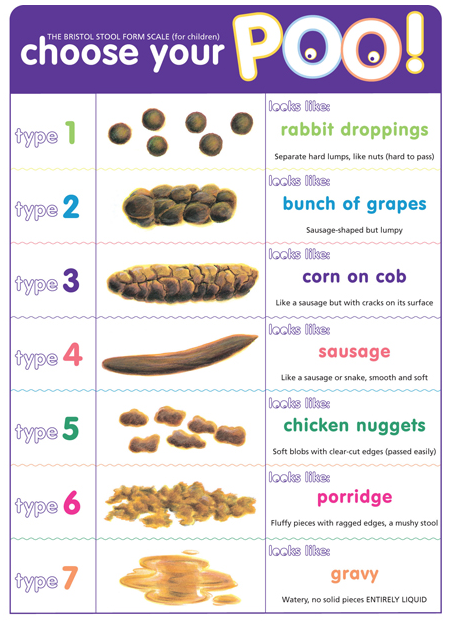
The Bristol Stool Chart for Children
Or you could make your own, like we did ;) Young children love toilet humour and humour is great for reducing tension and anxiety. Our own chart included "Jacket Potato Poo" and "Volcano Poo" amongst others, I will trade laughing over stress and anxiety any day.
The child who is presenting with rabbit dropping type stool or type 1 on the chart above would clearly benefit from more water in their stool. They may well not be drinking enough, and checking this is an excellent place to start. This type of constipation can also be a direct response to
food/gut allergies but the latter is more likely to slow motility than affect the water content in the stool. That my personal observation though, I am happy to be corrected on that one!
 Movicol
Movicol (or Miralax in the USA) is an osmotic laxative and a great drug for short term use in such cases (Type 1 stool) . It contains a plastic derivative that is used in disposable nappies (macrogol polyethylene glycol '3350) and just like the child who sits in a paddling pool with a nappy on, it swells with water. (try leaving a few sachets mixed overnight and see how it turns by morning.) This obviously DOES increase the water content..... but as you can see it will also increase stool volume.
My big concern is that this drug is the routine first line medication for childhood constipation. Have you checked out the racks of frequently used prescription meds in Boots? Movicol is probably taking up at least a whole round shelf.... and every GP in the country seems to have a Movicol sponsored sticky notes pad. Great marketing..... but this drug is really not ideal if you are NOT dealing with classic constipation.
Slow transit constipation can actually result from chronic untreated/poorly or inadequately treated classic constipation. The bowel can become stretched as hard stool collects as bowel peristalsis struggles to move it along. In this scenario Movicol can be helpful to soften the stool but it will increase the stool volume in high doses, thus giving the bowel even more work to do at a time it is struggling. It is important to explain to your Dr about your child's stool consistency and normal pattern of passing stool, because if you are straying into the slow transit category Movicol use needs some caution. This is especially important in young children because there is a balancing act between being as gentle as possible, clearing the bowel effectively to avoid compounding the problem and ensuring you are not adding to the problem if motility is an issue.
Slow transit will often happen in an inflamed bowel, which cannot contract and relax as effectively as it might do despite stool being a normal consistency. I have explained how local allergic responses to food in the gut can impact on bowel motility
here , in some there is a rapid response, if my youngest son ingested anything different as a baby his gut seemed to "switch off" whereas his twin sister would have a slower response, making it much more difficult to work out the trigger!
So the slow movement might be due to true constipation or it might be due to bowel inflammation (or other disease) but (and I had a recent discussion at GOS with our motility consultant about this) it is important to know as far as possible what you are treating, as high fibre/volume is not beneficial for a bowel which is struggling and when you are not dealing with a hard stool issue.
Dysmotility is slightly different. There are many different causes, and there are some excellent explanations
here . It might involve a muscle problem or a nerve problem, and sadly the latter can happen as a direct result of chronic constipation. Muscle and nerve problems can be picked up in a test called Colonic Manometry, a very useful (although only available at GOS in this country at present) test to determine nerve and muscle function in the colon.
This is one of the problems my son is dealing with. As well as having slow transit due to inflammation (EGID) he has nerve damage in his colon as a result from years of having an inflamed and overloaded bowel. We were at the point where he needed the highest dose of the one of the strongest stimulant laxatives (sodium picosulphate) and was still only able to "go" approximately every 9-10 days, at which point the volume was so enormous that he would block the toilet frequently. It's not exactly rocket science when it comes to understanding how a dysmotile bowel or one with slower motility might struggle with large doses of fibre and or Movicol. The 8-12 sachets per day we had to give for over two years appeared to us to be contributing to, not helping the problem. After careful discussion with his doctors we decided to stop the Movicol..... and held our breath. He started going almost every day - still requiring the stimulant laxative - which was the most fabulous step forward. For us, Movicol was NOT the answer, and I wished I had understood the difference between transit problems and constipation a lot earlier. Our son now has an overly large (diameter) and far longer colon than usual, as a result of years of overloading it. This has caused nerve damage (which may heal over time) which is probably more severe than it would have been had we addressed the motility issues a lot earlier. My youngest son has EGID, is more complicated than "normal" but nonetheless it took far too long to determine the cause of his "constipation" and get him on appropriate medication.
Hirschsprung’s Disease is an uncommon motility problem marked by an absence of nerve cells in the walls of the rectum or colon. This condition is present at birth and can be hereditary. Without the necessary nerve cells, intestinal contractions cannot occur, and stool remains trapped in the large intestine, called obstruction. Not passing meconium, constipation, and vomiting are common symptoms. Treatment is primarily surgical, with the removal of affected tissue from the bowel.
Lastly there is the
outlet obstruction type of constipation, where the stool consistency is not the issue, the motility is (initially) not the issue but the child has to strain and strain. This can be for different reasons. In the allergic gut, inflammation of the anal sphincter will inflame it and cause it to rest at a much higher pressure than normal. To pass stool, the sphincter pressure must be equalled from the other side, to cause it to relax. A sphincter at a very high pressure will require a large volume of stool (of whatever consistency) to be present to permit relaxation. The child will strain and strain and eventually pass a large volume of stool which might even be liquid but which cannot be passed until the volume creates sufficient pressure. Unfortunately this becomes a vicious circle, because the higher than normal volume needed eventually stretches the rectum and it becomes looser, so larger volume is needed to equalise the pressure and so on.
Anorectal manometry is really useful for testing this potential problem. In the USA Botox has successfully been used to treat this problem but identifying the inflammatory triggers and treating the inflammation is the way forward.
Young children can also have
functional constipation, such as withholding stool which should also be considered in a child of toilet training age. Whilst a behavioural issue it can cause longer term problems as you will work out from the info above. Stool collecting in any part of the colon over a long period is a potential problem and you should speak with your Health Visitor or GP.
Constipation of any sort will often impact on the entire GI tract. If one bit of the pipe functions less well, the rest will know about it. Reflux will be worse, abdominal pain is possible, reduced appetite with a feeling of fullness, and even retching and vomiting. This is very obvious in infants whose smaller bodies exhibit rapidly worsening reflux should they already suffer, and one reason why feed thickeners and so called "hungry baby" milks can make things so much worse. Digestion of solids and thickened milks takes longer, making the baby feel fuller for longer but allowing the stomach contents more time to reflux back. Hungry Baby Milk has no nutritional or calorific value over and above normal formula and is therefore only designed to make babies tummies feel fuller for longer presumably for the benefit of the parents, with potential problem resulting from delayed digestion for babies who already suffer with reflux.
If you are dealing with more severe motility problems there is an excellent article here in the Complex Child ezine.
As you can see, there is far more to "constipation" than needing to add water to the stool. It is important to have some idea of current stool consistency compared to your child's "normal" if consulting a doctor about it, and to initiate a discussion as to whether your child is going less frequently, having trouble passing the stool, and what that stool consistency is when coupled with those symptoms rather than merely reporting "constipation" and leaving the surgery with a box of Movicol sachets. There is a growing body of parents (and thankfully, doctors) who are concerned about the overuse and misuse of this apparently benign drug which I sincerely hope will avoid others going through some of the problems we have suffered, and still suffer today.
There is some excellent information here on constipation in children. Remember, Constipation can be very common in young children and occur for no obvious reason. (idiopathic) The information on this Blog is aimed at those parents managing children with underlying issues, such as allergic, inflammatory gut issues because that is the background I have, but in all cases of constipation in children careful note needs to be taken of the circumstances and symptoms.
DISCLAIMER - I am not a doctor, the information above I have ben told, read and learned over the years. The opinions are not only my own, but it must be stressed that this is a Blog not a medical document and whilst knowledge and opinion is useful you must follow the advice of your/your child's doctor. By all means discuss the above, I have carefully referenced the information but I am not medically trained.